

Contents
Development of the Sinus Venosus
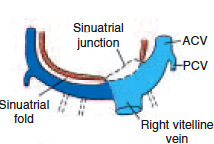
The sinus venosus receives venous blood from the right and left sinus horns in the middle of week four. The veins that supply this blood include the vitelline vein, the umbilical vein, and the common cardinal vein. At first, a lot of connection between the atrium and sinus occurs.
The sinus opening, on the other hand, quickly moves to the right. Blood shunts from left to right occur in the venous system during the fourth and fifth weeks of development, causing this shift. The left sinus horn quickly loses its relevance after the right umbilical vein and the left vitelline vein are obliterated during the fifth week.
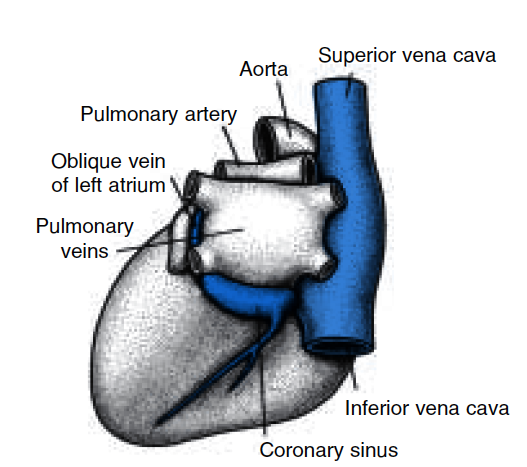
The oblique vein of the left atrium and the coronary sinus are all that remains of the left sinus horn after the left common cardinal vein is obliterated at 10 weeks (Fig1a&b).
The right sinus horn and veins grow dramatically as a result of blood shunts from left to right. The right horn is absorbed into the right atrium to form the smooth-walled section of the right atrium, which is now the only communication between the original sinus venosus and the atrium.
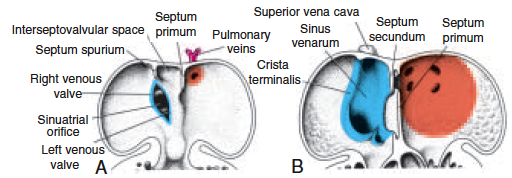
The sinu atrial orifice, which leads into the heart, is flanked on each side by a valvular fold, the right and left venous valves (Fig.2A). The valves unite dorso cranially, generating a ridge known as the septum spurium (Fig. 2B).
The valves are initially big, but the left venous valve and the septum spurium unite with the growing atrial septum when the right sinus horn is absorbed into the atrium wall (Fig.2C ). The right venous valve’s superior portion vanishes completely.
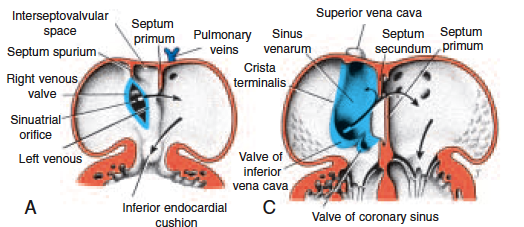
The right venous valve’s superior portion disappears completely. The inferior section develops into two parts: (a) the inferior vena cava valve, and (b) the coronary sinus valve (Fig. 2C ).
The crista terminalis separates the original trabeculated segment of the right atrium from the smooth-walled part (sinus venarum) that arises from the right sinus horn.
The Cardiac Septa’s Formation
Between the 27th and 37th days of development, as the embryo expands in length from 5 mm to around 16 to 17 mm, the primary septa of the heart are produced.
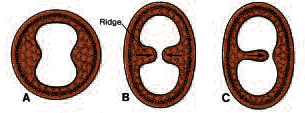
Two actively growing masses of tissue approach each other until they join, splitting the lumen into two distinct canals, and this is one technique of forming a septum (Fig. 3, A, B).
Such a septum may also be formed by active growth of a single tissue mass that continues to expand until it reaches the opposite side of the lumen (Fig.3C ).
The production and deposition of extracellular matrix, as well as cell proliferation, are required for the formation of such tissue masses.
Endocardial cushions form in the atrioventricular and conotruncal areas of the heart. They help construct the atrial and ventricular (membranous part) septa, the atrioventricular canals and valves, and the aortic and pulmonary channels in these places.
Septum Formation in the common atrium
A sickle-shaped crest rises from the roof of the common atrium into the lumen at the end of the fourth week. The first segment of the septum primum is this crest (Figs. 2 A and 4, A and B). The septum two arms reach toward the atrioventricular canal’s endocardial cushions.
The ostium primum is the space between the lower margin of the septum primum and the endocardial cushions (Fig. 4, A and B). Extensions of the superior and inferior endocardial cushions form along the septum primum margin as it develops, closing the ostium primum (Fig. 4, C and D).
Cell death causes perforations in the upper region of the septum primum before it is completely closed. The ostium secundum is formed by the coalescence of these perforations, providing unobstructed blood flow from the right to the left primitive atrium (Fig. 4, B and D)
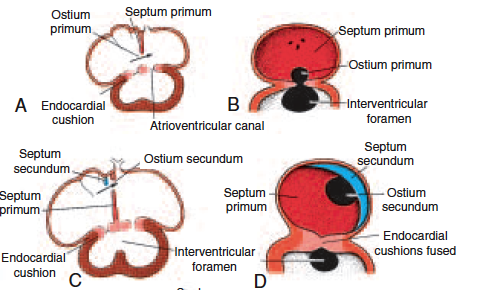
A new crescent-shaped fold emerges when the right atrium lumen widens as a result of the sinus horn’s integration. The septum secundum (Fig. 4, C and D) is a new fold that never creates a complete barrier in the atrial cavity (Fig. 4G ).
Its anterior limb in the atrioventricular canal extends downward to the septum. The free concave edge of the septum secundum begins to overlap the ostium secundum when the left venous valve and the septum spurium fuse with the right side of the septum secundum (Fig.2, A and B).
The oval foramen (foramen ovale) is the opening left by the septum secundum. The remaining segment of the septum primum forms the valve of the oval foramen as the upper part of the septum primum gradually fades.
An obliquely elongated fissure (Fig. 4, E–G ) connects the two atrial chambers, through which blood from the right atrium travels to the left side (arrows in Figs. 2B and 4E ). Newborns atria are separated by a thin structure called the interatrial septum, which is part of the valve of the oval foramen. When pressure in the left atrium increases, blood flow forces that valve against the interatrial septum and effectively removes the foramen from between the two atria.
In about 20% of cases, fusion of the septum primum and septum secundum is incomplete, and a narrow oblique cleft remains between the two atria. This condition is called probe patency of the oval foramen; it does not allow intracardiac shunting of blood.
Further Differentiation of the Atria
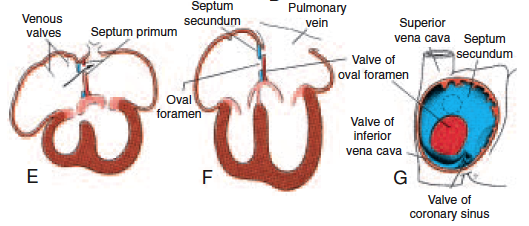
The primitive right atrium expands when the right sinus horn is incorporated, and the primitive left atrium expands as well. A single embryonic pulmonary vein emerges from the posterior left atrial wall, just to the left of the septum primum, at first (Fig. 5A).
This vein connects to the veins of the growing lung buds. The pulmonary vein and its branches are absorbed into the left atrium during development, resulting in the vast smooth-walled section of the adult atrium. Although only one vein reaches the left atrium at first, as the branches are integrated into the developing atrial wall, four pulmonary veins eventually enter (Fig. 5B).
The original embryonic left atrium is represented by little more than the trabeculated atrial appendage in the fully formed heart, whereas the smooth-walled section is derived from the pulmonary veins (Fig. 5). The original embryonic right atrium forms the trabeculated right atrial appendage, which contains the pectinate muscles, and the smooth-walled sinus venarum emerges from the right horn of the sinus venosus on the right side.
Reference: Text book of Embryology 9th edition, Moss and Adams. text book 4 edition, Braunwald Heart Disease, Grace Anatomy, Cardiac Science/HealthNactive