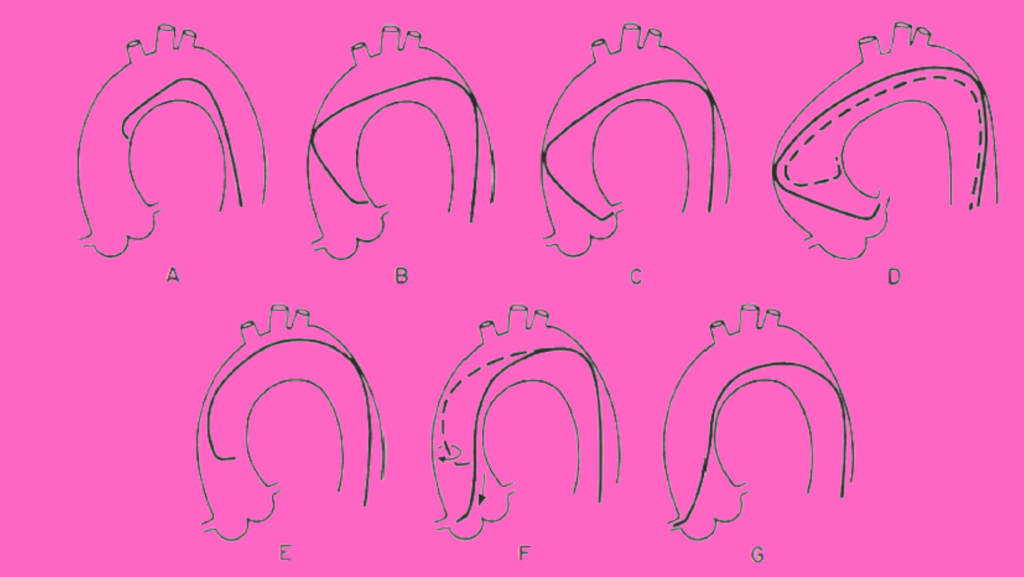
Angiogram, As of currently diagnostic coronary angiography remains the primary component of cardiac catheterization. The aim is to examine the whole coronary tree (both native vessels and any bypass grafts) while recording details of the coronary anatomy, including the following, the pattern of arterial distribution, anatomic or functional pathology (atherosclerosis, thrombosis, congenital anomalies, or focal coronary spasm), and the existence of inter-coronary and intra-coronary collateral links.
The procedure Angiogram is usually performed in 30 minutes or less, under local anaesthesia, on an outpatient basis, with a procedure related significant complication rate (death, stroke, myocardial infarction) of < 0 . 1 %. It is possible to define all portions of the coronary arterial circulation down to vessels as small as 0.3 mm, free of any artefacts due to vessel overlap or foreshortening, by performing a series of intra-coronary contrast injections in fully chosen angulated views using current high-resolution x-ray imaging.
Protocol
Articles Needed for Angiogram
- Puncture needle (18 Gauge)
- Introducer wire .038′ Teflon (45cm)
- 6F sheath (12cm) with dilator
- 0.035′ Teflon guide wire (145cm)
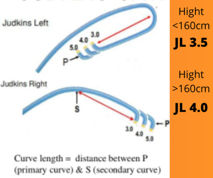
- Judkins Left 3.5 and Right Catheter 3.5 (6F)
")