Non-Fluoroscopy ICE Catheter Manipulation is an evolving technique, Compared to transthoracic and transesophageal echo, ICE has a number of benefits. Higher resolution and picture quality are possible because of the substantially shorter image distances created by the probe’s intra-cardiac position. In contrast to the difficult transesophageal echo probe, it can also be done without anaesthesia. These devices, which range in size from 8F to 10F, are capable of imaging in M-mode, 2D, 3D, and color Doppler. Both intra-arterial usage and use in veins are permitted for these catheters.
The selection of patients for ICE-guided interventions must take into account the size of the ICE catheters (require 8F to 11F sheathes). This can make vascular damage and access site issues more likely, or it might make the procedure more difficult for smaller patients. Technically, the tiny imaging field’s limitations must also be taken into account because they affect our capacity to see the entire interventional field.
Advancing the ICE Catheter
Obtain venous access via the left common femoral vein as usual. It is advised that a long sheath of at least 35 cm is used for direct access to the inferior vena cava because of the LFV’s typical tortuosity.
ICE Catheter View on Screen
The ICE catheter usually appears on the view screen from left to right when it is passing through the IVC. The catheter’s tip represents the head (on the right) and the leg (on the left) (Fig. a).

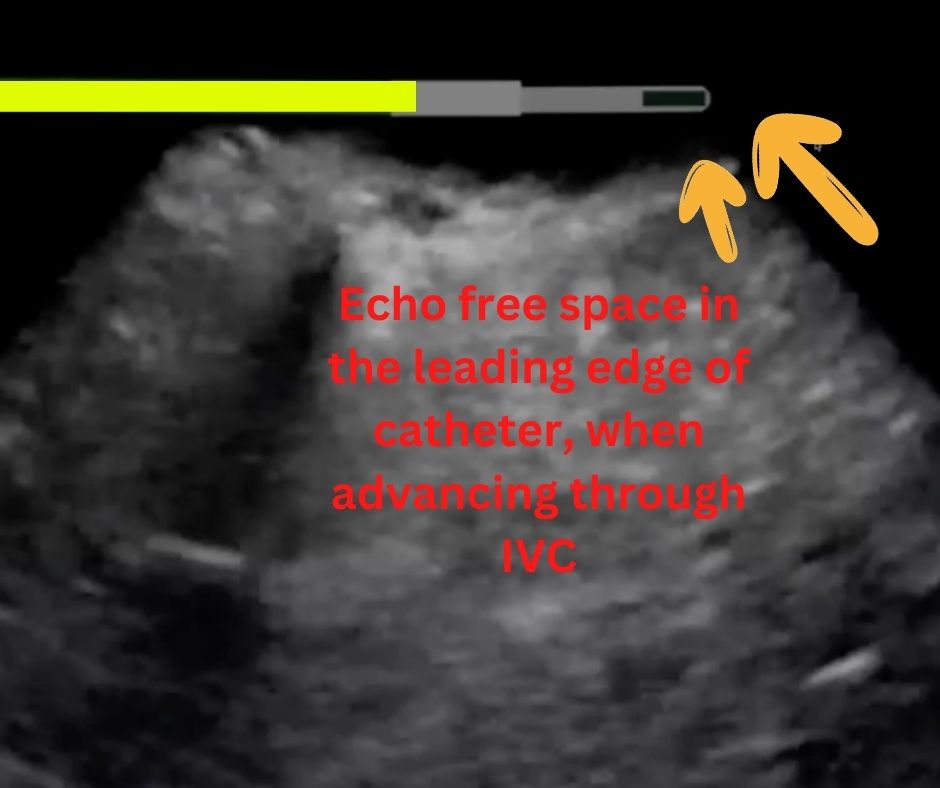
The leading edge of the ICE catheter is on the right side of the screen at about the 3 o’clock position and has an echo-free space. The catheter may be freely advanced throughout the arteries and cardiac structures by observing free space on its head. (Figure b).
Catheter Movement on IVC
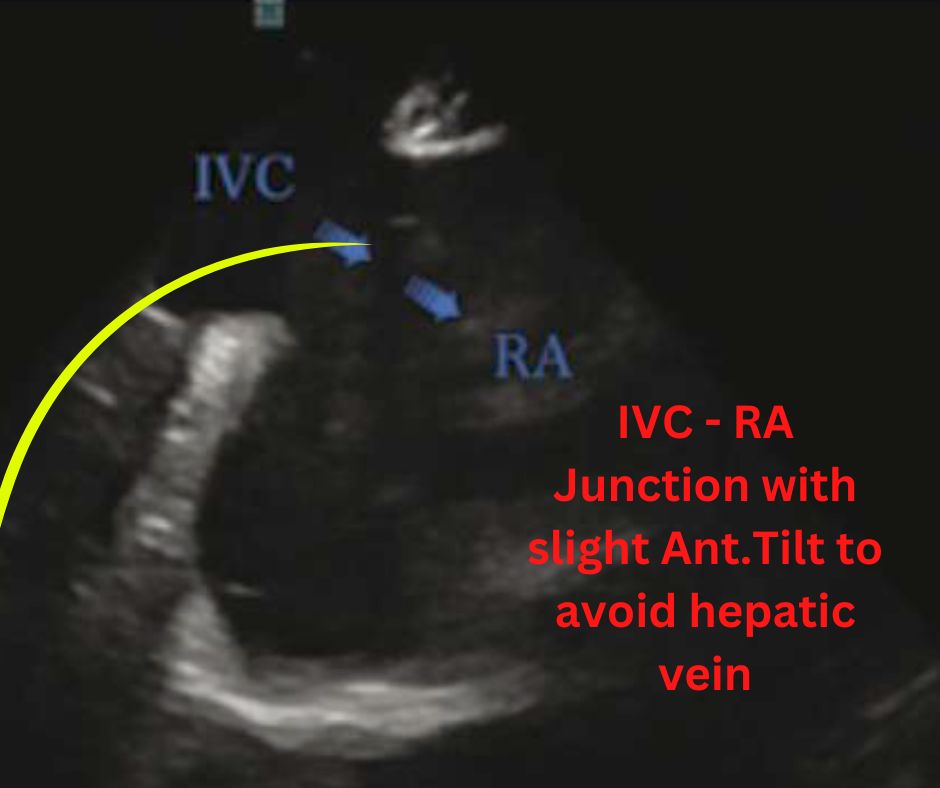
It is not always easy to pass the catheter through IVC because of its Anatomy. IVC is slightly slanted towards heart near liver and hepatic vein, to pass the catheter across this slant it is necessary to apply slight anterior tilt, which also makes the vein horizontal.
Please be aware that hepatic veins could be easily sub-selected, as indicated by hepatic tissue dominating the view screen. Usually, only catheter withdrawal and redirection with anterior tilt are needed to enter the RA. If there are problems advancing the ICE catheter, advance a different catheter from the same vessel that was accessed by the ICE catheter, such as the coronary sinus catheter, because it can give intracardiac electrograms showing that it is inside the heart.
Re-introduce the ICE catheter, track down the catheter with Clock Wise/Counter Clock Wise rotation as required, and follow that catheter to the heart. The bifurcation of vessels could be problematic as well. This can be avoided by using anterior tilt to guide the ICE catheter tip to the vessels’ junction. Apply minor CW/CCW rotation as required to keep the junction in view, then advance the catheter once the aperture is at the 3 o’clock position. The same principle may be implemented at the IVC-RA junction (Fig. c).
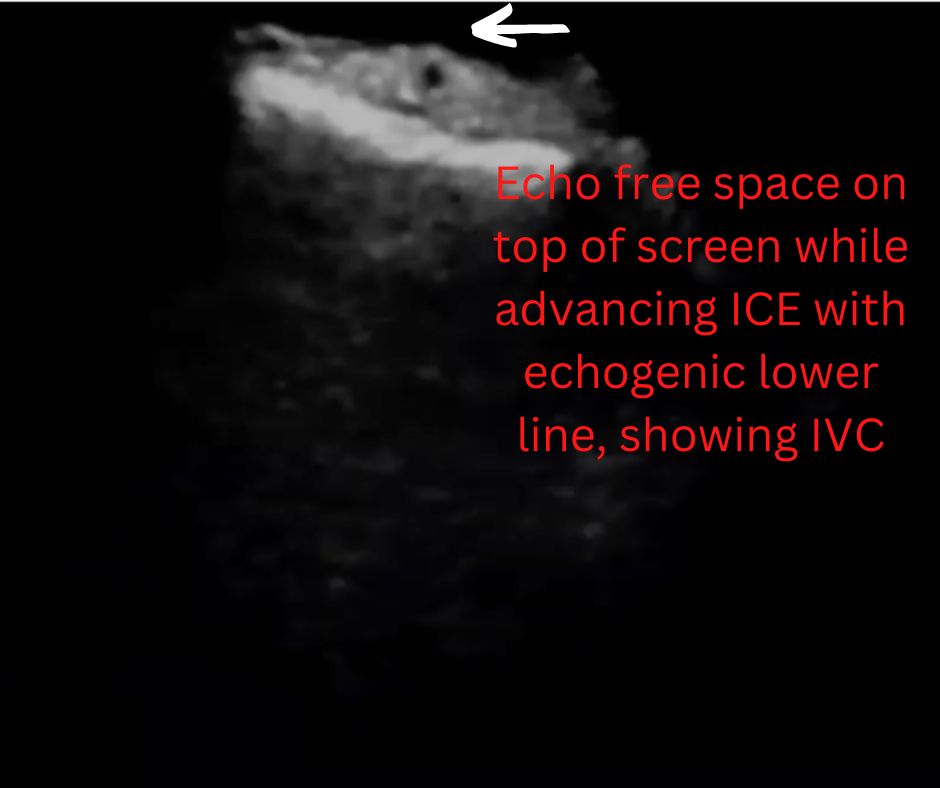
Appearance of IVC on ICE
IVC appears on top of the view screen horizontally. On the image, IVC appears as echo free space on top with an echogenic lower border (fig-d & e). The echo free space on the leading edge of the catheter needs to be closely monitored during its advancement.

Advancing ICE into RV
The ICE catheter is in the right atrium with anterior tilt. The catheter will dive into the right ventricle. Anterior tilt is the common method to cannulate the right ventricle with an ICE catheter. In the initial home view, the ICE transducer is in the right atrium and visualises tricuspid valve, right ventricle, and RVOT horizontally (top to bottom) on the view screen (fig-f). The moment the ICE catheter enters the right ventricle, it will bring the RV to the 3 o’clock position (fig-g).


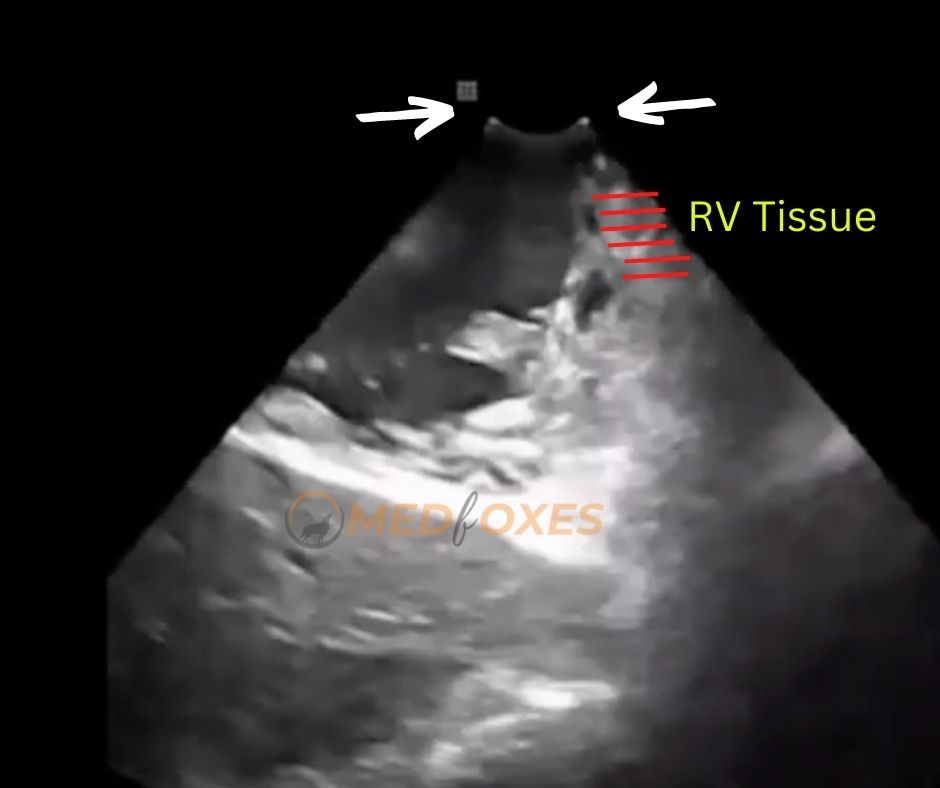
Pay attention to the transducer position during ICE catheter movement in the heart. The ICE catheter transducer can be seen on top of the image (fig-h) on the view screen. During catheter movement, the appearance of RV tissue at or beyond the tip mark of the transducer indicates the tip catheter is in close contact with the ventricle wall (fig-i), which leads to perforation. At this point, it is mandatory to relax the catheter by withdrawing.