

Unplanned PCI post TAVI is uncommon, and the incidence decreases over time. In the first two years following TAVI, acute coronary syndrome is the primary rationale for PCI; thereafter, chronic coronary syndromes are more common. Balloon-expandable and self-expandable bioprostheses appear to have no differences in the frequency or success of unplanned PCIs after TAVR.
Hardware’s Needed
- Puncture needle (18 gauge)
- Introducer wire .
- 038′ Teflon (45cm)
- Sheath 6F Femoral or Radial
- 035 J Teflon Wire6F or 5F
- Judkins, Left 3.5 or Judkins, Right 4.0
- 6F Pigtail Catheter.
Preparation
Femoral Approach (PCI Post TAVI)
- Sterile Trolley Preparation
- Antimicrobial painting (from umbilicus to knee joint)
- Draping the patient in such a way that the inguinal fold lies diagonal to the side hole
- Load 10ml of Xylocaine in a 10 ml BD syringe and Heparin 2500 I.U. in a 5 ml BD syringe.
Radial Approach (PCI Post TAVI)
- Sterile Scrubbing, Gowning, Gloving
- Preparation Of Sterile Trolley
Hand position need to done properly – Positioning of the hand for Trans-radial access. The hand is hyper-extended with use of a rolled towel behind the wrist and tape holding the fingers or with use of a dedicated positioning splint.

Painting – from middle ventral part of forearm to elbow and femoral region.
- Load 5ml of Xylocaine in 5ml BD syringe and Heparin 2500 I.U in 5 ml BD syringe
Prepare manifolder (Femoral & Radial)
- First port with Pressure line
- Third port with contrast
- Attach 10ml luerlock syringe
Steps
6 French access from the femoral or radial (left radial is preferred) artery as per the operator’s experience.
Use J-wire to enter the diamond in front/adjacent to the coronary ostia.
Use stiff angle glide wire when there is difficulty entering diamond or tracking the catheter.
Commissural post in front of Coronary ostium (Suppose you are unable to enter the diamond in front of the ostia.)
Left Coronary Artery
- Advance JL3.0 or JL 3.5 Guide catheter
- Aortogram is also helpful if it is not possible to selectively cannulate the left coronary artery.
- Second choice is to using a guide catheter Ikari Right 1.0/1.5
- Coronary guide wire, Balloon Support, or Guide liner can be used if there is difficulties in Selective engagement of Ostium
Right Coronary Artery
- Advance JR4 Guide Catheter
- Second choice is to use guide catheter: Ikari Right 1.5 or Multipurpose (MP)
- Coronary guide wire, Balloon Support, or Guide liner can be used if there is difficulties in Selective engagement of Ostium
Commissural post away from coronary ostium (Assume that you can access the diamond at the level of the coronary ostia)
Left Coronary Artery
- Advance JL3.5 or JL3.0 Guide catheter
- Second option is to use guide catheter: Ikari Right 1.0/1.5
- If skirt is high, use Ikari Right 1.0/1.5 guide to enter from diamond above coronary ostia
- For difficult cannulation Balloon support, Coronary wire or guide liner can be used.
Right Coronary Artery
- Use JR4 guide Catheter
- Second option is to use Ikari Right or Multipurpose guide catheter (Particularly if wide sinuses)
- If skirt is high, use multi-Purpose guide catheter to enter from diamond above coronary ostia.
- In case of difficulties in advancing guide catheter and placing it Co-axial balloon Support, Coronary wire or Guide liner can be useful.
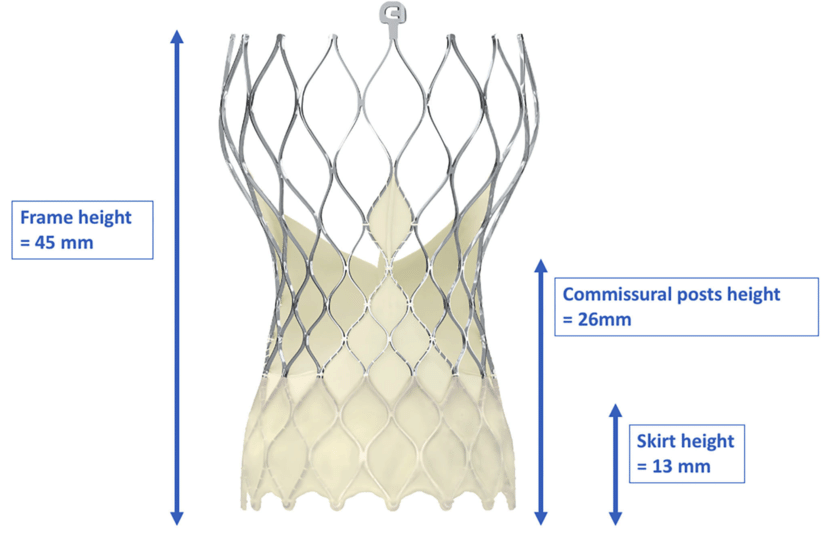
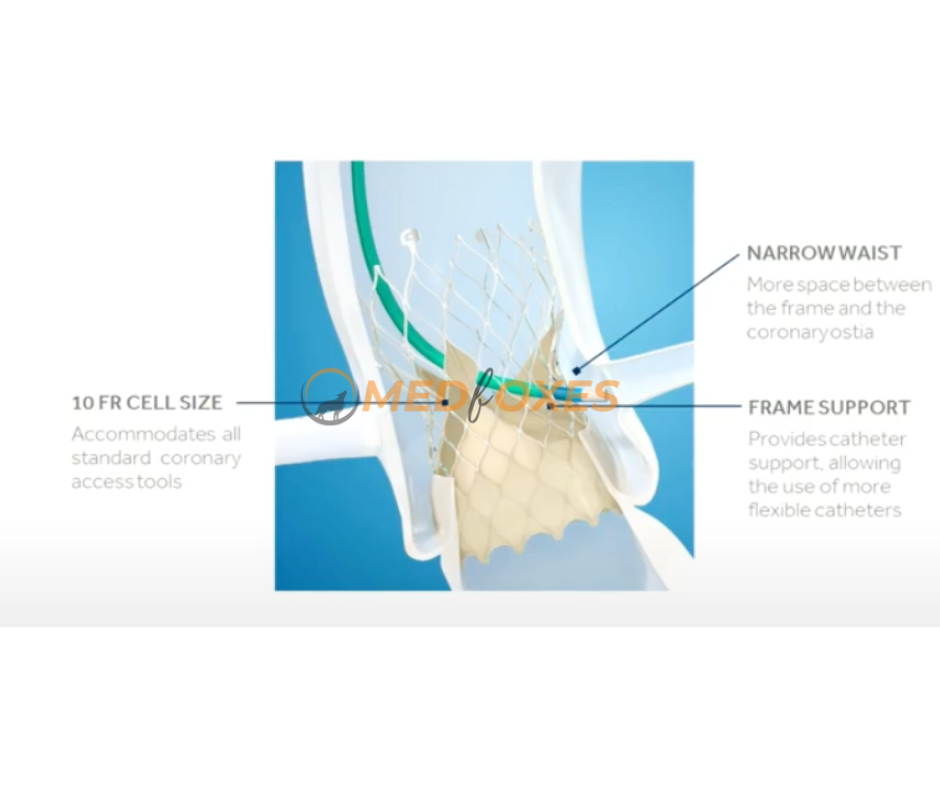
The architecture of Core Valve, particularly its narrow waist, cannulation of the Left Coronary Artery typically requires a smaller catheter than regular. For femoral and radial access, respectively, JL3.5 and JL3.0 catheters are available for LCA cannulation. The LCA and the narrow waist can both be addressed with a JR4. The site of the commissural post, which typically involves entering through the valve from a diamond above and/or lateral to the coronary ostia, is a crucial factor to consider. As a result, the Ikari right guide catheter is the preferred second-line catheter for left coronary engagement. Furthermore, if more selective engagement is required to perform a diagnostic angiogram, using a guide catheter as a backup option offers the prospect of coronary wiring, balloon support, or guide liner.
For left coronary intervention, a femoral left 3.5/3.0 guide catheter is the ideal guide. Extra backup catheters should only be used with the utmost caution since they have been linked to kinking. When there is substantial space between the valve frame and the ostia due to a large sinus of Valsalva, an AR2 guide is the preferred option rather than a JR4 guide catheter for right coronary procedures.
A downward-pointing catheter, such as a multipurpose guide, can also be employed, especially for RCAs, when the coronary ostia can only be reached from above.
Catheter engagement.
Depending on how the skirt and commissural posts are positioned in relation to the coronary ostia, selective catheter engagement may be challenging. Coaxial cannulation through the diamond right in front of the ostia is preferred whenever possible. Engaging from a diamond below the ostia has been associated with kinking of the guide and the failure to remove it. In order to avoid being obstructed by the native valve leaflets or the pericardial tissue that extends from the base of the frame, operators have found it helpful to cannulate at the fifth alternating diamond above the base of the frame.
A J-wire is very useful in locating the diamond adjacent to the ostia, and the catheter can be railed over it for cannulation and angiography. If this doesn’t work, a stiff, angled glide wire can be used in the same way. It can more easily enter the diamond of the valve frame at the ostium because it is more lubricious, and since it is stiffer, the catheter can be straightened as it is railed across the diamond. Despite the fact that the angled tip offers some protection, due to the close proximity of the left major coronary artery, it should always be used with caution.
If selective engagement is still a challenge, the coronary artery can be accessed from the aorta using a coronary wire, which can then serve as a rail for the guiding. A 2.0 mm X 12-mm balloon can be positioned in the left major coronary artery to provide additional support if guide cannulation and support are still insufficient. This is done while attempting to rail the guide over the balloon. If that doesn’t work, a guide liner catheter can be introduced, with balloon supported tracking in the most challenging situations.
Catheter disengagement.
The guide can kink throughout the procedure, therefore it needs to be carefully disengaged. As a result, the guide needs to be detached from the ostium, ideally over a wire, before being pulled out via the valve frame’s diamond. Excessive force must be avoided if this proves challenging because it can kink or even break the catheter over the valve frame. A balloon may be used to support disengagement and withdrawal from the valve frame if necessary.