
Balloon Mitral Valvuloplasty is an Interventional treatment used to increase the opening of a narrowed (stenotic) valve
The most common cause of native mitral stenosis is rheumatic heart disease. The obstruction to inflow resulting from fusion of the valve commissures is the pathophysiologic problem in these patients. Left atrial hypertension, atrial arrhythmias, pulmonary hypertension, and congestive heart failure are all symptoms of progressive rheumatic mitral stenosis, which can develop decades before clinical manifestation.

Patient Selection for Balloon Mitral Valvuloplasty
By separating the commissures without damaging the leaflets or supporting apparatus, successful Balloon Mitral Valvuloplasty relieves mitral stenosis. The accurate assessment of valve morphology, which should include the mechanism of commissural fusion, the pliability of the valve, and the status of the sub valvular apparatus, is therefore critical to procedural success. A successful result from balloon mitral valvuloplasty may be hampered by severe retraction and fusion of the chordae and papillary muscles. The Wilkins score, in which points 1–4 are allocated based on the physical properties of the valve, is a standard method for echocardiographic assessment.
Hardware’s Required
- 6F Arterial Sheath
- 9F Venous sheath
- 6F Multi Purpose catheter with 0.035-terumo wire (150cm)
- 6F Pigtail with .035 Teflon wire (145cm)
- Mullins sheath with .032 wires (145cm)
- Septal puncture needle or broken bro needle
- LA wire or Jalebi guide wire
- Septal dilator (12F)
- PTMC Balloon {Percutaneous Transluminal Mitral Commissurotomy}
- Accura or Inoue Balloon, selected according to the patient height

The Formula for balloon size
Balloon Size =Height / 10 +10
E.g: 160 cm / 10 =16 +10 ==> 26
So size to be selected for the patient with 160cm is =26mm

- Balloon stylet both inner and outer
- Two pressure line with 3-way stopcock
- Contrast- Bowl of non-ionic for Septal Puncture
- Bowl of ionic contrast 1:5 dilutions for balloon preparation
- LV stylet
- Balloon syringe
- Vernier scale
Disposable Items
10cc BD syringe- 1
10L/L syringe -2
3-way 10 cm extension – 1
5cc BD syringe – 1
21 Gauge long needle – 1
11# Blade – 1
3-way-stopcock -1
Balloon Preparation
- Take 10 ml of Ionic Contrast in a bowl and dilute into 1:4 dilution (10 ml of contrast in 40 ml saline)
- Aspirate the diluted contrast in 25cc balloon syringe (Comes with balloon)
- Attach balloon syringe with 10 cm extension fill that with contrast
- Flush the inner port of the balloon and attach the syringe in balloon port
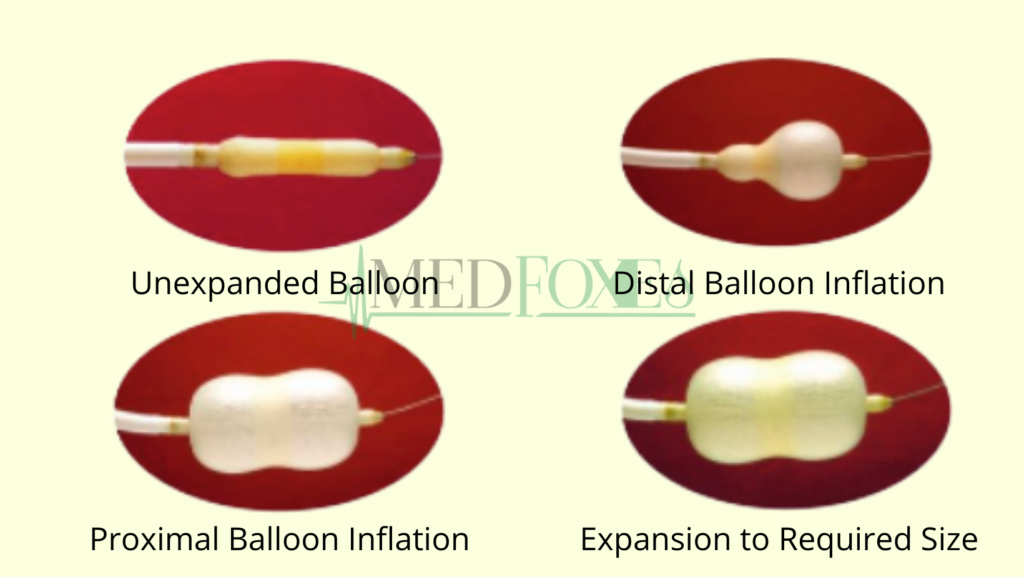
- Inflate the balloon and keep the balloon upside down then deflate it fully (repeat it again)
- Remove the air from syringe and inflate the balloon, close three-way and measure the balloon with Vernier scale
- Once the balloon is inflated up to required size remaining contrast in syringe should be discarded
- Deflate the balloon fully and insert inner stylet of the balloon when the 0.032 Guide wire is well into the balloon
- Attach the inner stylet with outer stylet and then push both into balloon (Don’t Push the one stylet alone, it will damage the balloon)
- Flush inner port and keep it ready for use.
Procedure Steps
- Obtain arterial and venous access, introduce 6fr sheath for artery and 9fr sheath for venous
- Flush the sheaths and connect the pressure line to the arterial sheath
- Introduce Multi-Purpose or RCA catheter or Swan Ganz catheter through venous sheath into the PA for pressure measurement
- Change the recording scale depends on pressure to get clear Pressure tracing’s
- Introduce pigtail catheter with 0.035 Teflon guide wire to the LV and ascending aorta for measurement of LV pressure and pull back of ascending aorta Pressure, Once the pressure recording done, keep the catheter in Ascending Aorta with pressure attached (It serve as landmark for Aorta During Septal Puncture)
- Replace the Multi-Purpose catheter with Mullen’s sheath. It should be introduced with 0.032 Teflon guide wire
- When the guide wire reaches the left subclavian vein remove the guide wire and the sheath Dilator
- Introduce septal puncture needle into the Mullen’s sheath with 10cc L\L syringe of non-ionic dye
- Once septal puncture is done, inject contrast and see whether it is opacify LA and Pulmonary veins, then remove the needle introduce LA wire in to the LA
- Inj. Heparin 5,000 IU/IV to be given immediately once LA is approached.
- Remove the 9F venous sheath, Mullin’s sheath and let the LA wire remains in Left atrium
- Now # 11 Blade and Artery forceps to be used to dilate skin and under structure
- Wipe the LA wire with wet gauze
- Advance the 12F dilator to dilate skin and septum over LA Wire
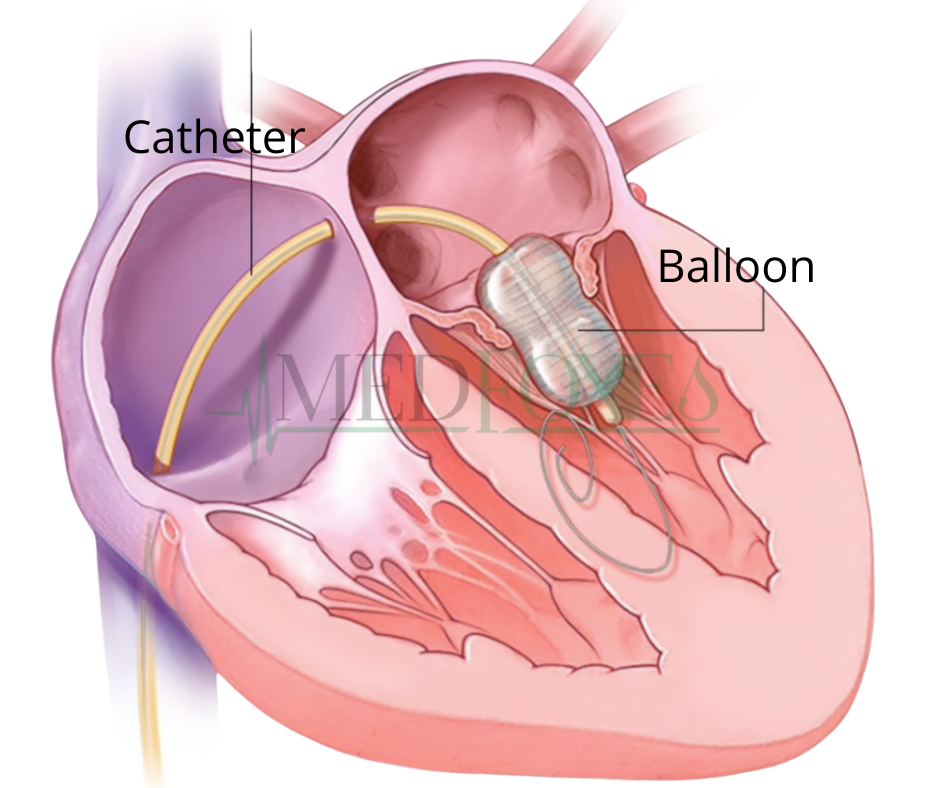
- Replace dilator with prepared BMV balloon into LA and remove the LA wire along with inner stylet and attach the balloon syringe, then inflate the distal balloon slightly
- Put the LV stylet into the balloon to introduce the balloon into LV across the mitral valve
- Once the balloon crossed the valve inflate the distal portion and see whether the balloon is holding the valve
- Inflate the balloon without waist to stretch the Mitral Valve and deflate the balloon as soon as possible
- Remove the balloon from the LV to LA; attach the pressure line and flush. Note LA pressure and aortic pressure
- Introduce the LA wire with inner stylet of the balloon and remove the balloon, let the LA wire is inside the LA
- Put the same 9F venous sheath to maintain haemostasis, do post study of PA pressure
- Remove both venous and arterial sheath, apply pressure bandage and shift the patient to ICU.