
Following TAVI, coronary interventions can be technically challenging. The selective cannulation of the coronary ostia, which is dependent on patient anatomy, valve type and design, and implantation parameters including implantation depth and the orientation of the commissural tabs with respect to the ostia, is the most difficult part of the surgery. The following, we summarise the technical aspects of CAG for the different valve types.
Hardware’s Needed
- Puncture Needle (18 gauge)
- Introducer wire .
- 038′ Teflon (45cm)
- Sheath 6F Femoral or Radial
- 035 J Teflon Wire6F or 5F
- Judkins, Left 3.5 or Judkins, Right 4.0
- 6F Pigtail Catheter.
PREPARATION
Femoral Approach
- Sterile Scrubbing, Gowning, Gloving
- Sterile Trolley Preparation
- Antimicrobial painting (from umbilicus to knee joint)
- Draping the patient in such a way that the inguinal fold lies diagonal to the side hole
- Load 10ml of Xylocaine in a 10 ml BD syringe and Heparin 2500 I.U. in a 5 ml BD syringe.
Radial Approach
- Sterile Scrubbing, Gowning, Gloving
- Preparation Of Sterile Trolley
Hand position needs to be done properly – Positioning of the hand for trans-radial access. The hand is hyper-extended with the use of a rolled towel behind the wrist and tape holding the fingers or with the use of a dedicated positioning splint.

- Painting-from the middle ventral part of the forearm to the elbow and femoral region.
- Load 5ml of Xylocaine in a 5ml BD syringe and Heparin 2500 I.U. in a 5 ml BD syringe.
Prepare manifolder
- First pressure line port
- Third, a contrast port
- Attach a 10ml luerlock syringe.

Steps
- 6 French access from the femoral or radial (left radial is preferred) artery as per the operator’s experience.
- Use J-wire to enter the diamond in front/adjacent to the coronary ostia.
- Use stiff angle glide wire when there is difficulty entering diamond or tracking the catheter.
Commissural post in front of Coronary ostia (Suppose you are unable to enter the diamond in front of the ostia.)
Left Coronary Artery
- Advance JL3.5 or JR4 catheter
- If not able to selectively cannulate the Left Coronary Artery perform non-selective angiogram, Aortogram is also useful
- Second option, using a guide catheter, FL3.0 or Ikari Right 1.5/1.0
- A guide catheter can be used with a coronary guidewire to wire the coronary artery for more selective engagement.
Right Coronary Artery
- Advance JR4 Catheter
- If not able to selectively cannulate the Right Coronary Artery perform non-selective angiogram, Aortogram is also useful
- Second Option, use guide catheter: Ikari Right 1.5 or Multipurpose (MP)
- Guide catheter can be used with a coronary guidewire to wire coronary artery for more selective engagement
Commissural post away from coronary ostia (Assume that you can access the diamond at the level of the coronary ostia)
Left Coronary Artery
- Advance JL3.5 or JR4 catheter
- Angiograms that are selective or semi-selective are typically diagnostic.
- Second attempt, use guide catheter: Ikari Right 1.0/1.5
- If skirt is high, use FR 4 or Ikari Right 1.0/1.5 guide to enter from diamond above coronary ostia
Right Coronary Artery
- Advance JR4 Catheter
- Angiograms that are selective or semi-selective are typically diagnostic.
- Second line, use Amplatz Right II catheter (Particularly if wide sinuses)
- If skirt is high, use multi-Purpose guide catheter to enter from the diamond above the coronary ostia
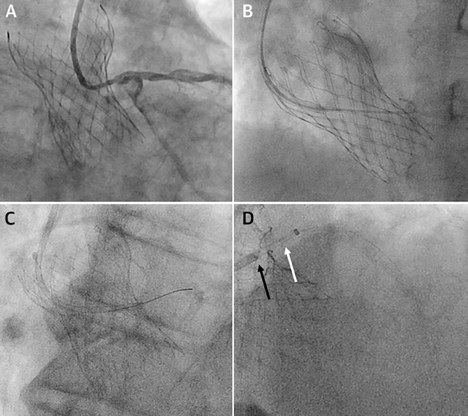
(A) JR4 was used to successfully engage the left main coronary artery. (B) The lowest diamond above the skirt is crossed with J-wire. (C) Coronary wire placed in the coronary artery before railing the guide for selective engagement. (D) The guide could not pass the valve frame. (black arrow), so a guide extension catheter (white arrow) was used to selectively engage the coronary artery.
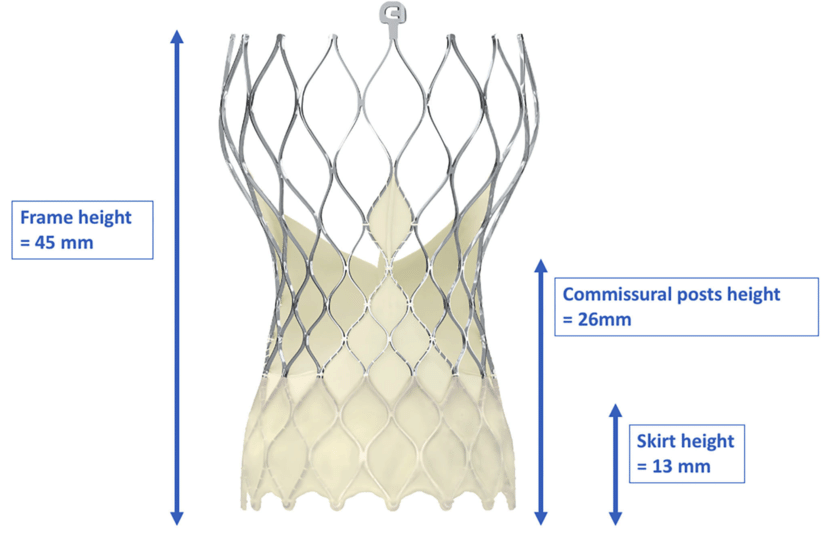
The design of the core valve, especially its narrow waist, cannulation of the left coronary artery usually requires a smaller catheter than usual. For LCA cannulation, JL3.5 and JL3.0 catheters can be used for femoral and radial access, respectively. A JR4 can also be used to engage the LCA and address the narrow waist. An important element to take into account is the position of the commissural post, which normally requires entering through the valve from a diamond superior and/or lateral to the coronary ostia. Consequently, the second-line catheter of choice for left coronary engagement is the Ikari right guide catheter. Furthermore, using a guide catheter as a second alternative provides the possibility of coronary wiring if more selective engagement is needed to carry out a diagnostic angiogram.
For RCA cannulation, JR4 is the catheter of preferred. Longer-tipped catheters, such as an AR2 (recommended), JR4.5, JR5, or an Ikari right guide, provide more effective engagement when the sinus of Valsalva is wide. A multipurpose catheter or an Ikari right guide is suggested if a commissural post is in front of the coronary ostium.
Catheter engagement
Depending on how the skirt and commissural posts are positioned in relation to the coronary ostia, selective catheter engagement may be challenging. Coaxial cannulation through the diamond right in front of the ostia is preferred whenever possible. Engaging from a diamond below the ostia has been associated with kinking of the guide and the failure to remove it. In order to avoid being obstructed by the native valve leaflets or the pericardial tissue that extends from the base of the frame, operators have found it helpful to cannulate at the fifth alternating diamond above the base of the frame.
A J-wire is very useful in locating the diamond adjacent to the ostia, and the catheter can be railed over it for cannulation and angiography. If this doesn’t work, a stiff, angled glide wire can be used in the same way. It can more easily enter the diamond of the valve frame at the ostium because it is more lubricious, and since it is stiffer, the catheter can be straightened as it is railed across the diamond. Despite the fact that the angled tip offers some protection due to the close proximity of the left major coronary artery, it should always be used with caution.
If selective engagement remains to be problematic, a coronary wire may be used to access the coronary artery from the aorta, and then it can act as a rail for the guidance. If guide cannulation and support is still inadequate, a 2.0 mm X 12-mm balloon can be positioned in the left main coronary artery for added support while trying to rail the guide over it. If that doesn’t work, a guide extension catheter can be introduced, with balloon-assisted tracking in the most challenging situations.
Catheter disengagement
The guide can kink throughout the process, so it should be carefully disengaged. Thus, the guide should be disengaged from the ostium, ideally over a wire, before being pulled through the diamond of the valve frame. If this becomes difficult, using excessive force must be avoided, as it can kink, or even break, the catheter over the valve frame. If needed, the use of a balloon may further support disengagement and withdrawal from the valve frame.
Also Read: How can coronary access be improved after TAVI?, Angiogram Radial Approach, Angiogram Femoral Approach